The term “frontline workers” often conjures images of doctors in Hazmat suits and soldiers in uniform. But during the coronavirus outbreak, workers across a vast array of industries have found themselves essential parts of the machine that keeps the world in motion, required to do their jobs despite great risk—whether hog farm employees or bus drivers, mental health counselors or police officers. Here, as part of TIME’s new issue, frontline workers of all types share their triumphs and fears in their own voices.

Andre Anglin, 51, bus driver in Columbus, Ohio
I start at 6:45 in the morning, and I usually get off around 6:30 p.m. Before 12 o’clock, it’s like a ghost town. But after 12 o’clock, people start coming out. I greet almost every passenger that comes on. Most people are going to loved ones’ houses to check on them. There’s a few people that might be going to the grocery store. And some people have essential jobs they have to go to.
I feel proud to be able to do my part, especially for the ones that may be going to the hospital because they’re worried that they have it, so they can get checked out. I was in the military, so I still have that sense of honor. I want to do everything I can to make sure that people are taken care of and protected. My employer moved the standing line back so that we’re kind of in an isolated area, and people are now coming in and out the backdoor, so there’s no more up-close personal contact with people coming near the fare box. I also make sure that I’m keeping myself sanitized and everything, but I feel more proud about helping other people than, at this moment, my own safety.
When I was in [the Gulf] war, I was in an aircraft carrier and it was actually stressful in the same way. This is an enemy that we really don’t have a full understanding of. So we’re doing our best to fight something that we don’t know, and I’m just trying to do my part. I also learned especially going to war that a smile can go a long way to making people feel better about everything that’s going on.
I was talking to a gentleman yesterday and he was like, “Without y’all, this city would be shut down.” And he said he wished he could do something special for us. But you know, I thought that him saying thank you was enough for me. —As told to Abby Vesoulis

Prince Paul Butau, 28, is the senior resident medical officer at Parirenyatwa Hospital in Harare, Zimbabwe
At my hospital we are closed to all outpatient and non-emergency services. We are not a COVID-19 hospital, so the government says we do not need protection equipment. So we only get two masks and a paper apron a day. We have goggles, but we have to sanitize them every day with alcohol. We should have full gear. The feeling among us junior doctors is that this is not enough. I don’t want to risk my life seeing a patient in casualty if I don’t have protection.
We don’t know who has COVID or not. Zimbabwe has only tested about 200 people, and they say there are only 11 cases. But I think the government is not being transparent, and it hasn’t done enough to contain the outbreak. I think the numbers are much higher. I am worried that it might explode like in Italy or Iran, but I am just praying it won’t be as bad, because if it explodes like it did in the U.S., I can’t describe in words what it will be like here.
There are only a few ventilators in the public hospitals, maybe less than 20 in the whole country. We have one COVID case who died. He was 30. He died because there was no ventilator at his hospital. His family brought one privately, but there was no electricity socket in his room, and they couldn’t plug it in. It shows how unprepared we are as a country. If there was a functioning system, he would have been fine. If we were not prepared for that one case, how can we handle more?
If we can’t stop it, if we can’t treat it, I am afraid we will become the next example of just how bad an outbreak can be. But I fear it will be even worse here. It will be the absolute worst-case scenario in the world. In the future, people will point to Zimbabwe and say, that is how bad an outbreak can be. —As told to Aryn Baker

Dennis Canale, 43, is a physician assistant at Staten Island University Hospital Northwell and NYPD detective Second Grade
For the past 16 years of my 22 year career I’ve been assigned to the NYPD’s emergency service unit. ESU is an elite SWAT rescue team in the country. We do everything from typical tactical SWAT work, which includes barricaded hostage jobs, or emotionally distressed individuals that need rescuing, to high angle road rescue to water rescues to the simple response for medical aid in car accidents with people trapped in vehicles. So we encompass a lot of different areas in that unit. I’m a Board certified and licensed Physician Assistant for the past 17 years, working in emergency medicine, surgery, and various other specialties.
I’ve been through several terrorist events here in the city, unfortunately I’ve been through 9/11, I worked down at Ground Zero for several months. I worked out here in Hurricane Sandy. I’ve watched my colleagues as first responders dive right in, no regard for their own safety, just for the wellbeing of others.This pandemic kind of took me in a different light. Right now I’m talking to you, life seems fine. It doesn’t really hit me until I walk into the hospital and see the amount of critically ill patients. It’s extremely surreal. I can remember pulling into Ground Zero the night of the towers and thinking I’m on a movie set. And the same thing here, it feels like a Hollywood movie with people in protective gear that you would never dream of in a hospital setting.
Our hospital asked for volunteers of personnel who would like to go help out at the COVID-19 testing tents, so I put in for it. I watched one lady pull up and she saw us come to the car all dressed up and she just started crying. And I looked at the people around me, all the professionals, and I’m like, it looks like a horror movie. How scary and how unsettling it must be to have to go through this as a normal person who lives your life happy, no worries… then you’re driving through a tent seeing people dressed up coming at you for swabbing and wondering, “What’s going to happen to me?”
Even the kids come through with their family. You can’t really talk to them because the windows are up, so the staff there was trying to laugh and wave at them. It’s very hard when you have a mask and a shield and a hood and everything else on, nobody can see your facial expressions. I had several people giving prayer hands and a nodding gesture saying thank you, thank you, and they give you the heart sign, and saying thank you so much, thank you so much, god bless you. People complain about the world, but you really see how appreciative people are. And it makes you feel good at what you do. It makes you say alright, I’ll go back tomorrow.
The most impressive thing that I see is the staff I work with. People who didn’t sign up in the medical field: the physician assistants, the doctors, the nurses, and most importantly the people that clean and repair, the people that are clerical, the people that help all the medical professionals. They didn’t take that job thinking, ‘Hey, I’m going to go out today and put my life on the line.’ I know that as a law enforcement officer I am going to run the risk of death. I know it every day. They don’t. But they’re all there doing it. It’s amazing to watch.
When I leave there and you’re alone for the drive home you think about well what if I get sick? What if I end up in the hospital or if I end up on that ventilator? What happens to your family? That’s when it starts devastating your mind. When I get outside the house it’s basically disrobing into a bag. It goes into a washing machine, and you take a shower. At my parents’ house, we talk to them from outside. I won’t even go in the same room with them because they’re older. Around my family, I wear a mask.
You keep saying to yourself, eh, tomorrow it’ll be over. Tomorrow it’ll be over, tomorrow it’ll be over. But the estimation right now is tomorrow it will be worse. —As told to Paul Moakley

Luigi Cavanna, 67, is the head of the oncology ward at Guglielmo da Saliceto hospital in Piacenza, Italy
In early March, when the epidemic hit, the situation in the E.R. was extreme. People were coming in all the time, dozens of them, already in serious condition. Beds and stretchers everywhere.
One of my patients was in the E.R. for 10 hours and then she signed a paper stating that she wanted to be taken home. She said she’d rather die in her own bed. So I visited her at home and gave her some medicine. Within a few weeks, she got better. That’s when I realized we shouldn’t be waiting for the COVID-19 patients to get to the hospital. We needed to go to people’s homes, even of those with mild symptoms, and treat the disease before it could get worse. In the beginning the rallying call was to increase the number of hospital beds and all our efforts were directed towards that objective, but in doing so we were overlooking the territory.
We’ve got to remember that COVID-19 is not a heart attack or a stroke. It follows its course, and we must stop the action of the virus before the lungs are too seriously damaged. If you enter the spiral of the hospital already in serious condition, you don’t always manage to leave. I started to drive around the area surrounding Piacenza with my staff on March 10, and initially we visited as many as 15 people a day. Then we gradually became better organized, and now we have three teams and we continue to work also in the hospital.
When we go to patients’ homes, we do a chest ultrasound with a device the size of a cell phone, but no swabs. In this area, anyone who shows the typical symptoms of COVID-19 is almost certainly positive. We leave the swabs for later, when patients have recovered, to make sure they’re no longer contagious. Up until April 2, we left two medicines to be taken by mouth, hydroxychloroquine commonly used for rheumatoid arthritis and an antiviral used for HIV. Then AIFA [Italy’s equivalent to FDA] issued a note advising us to be very careful in prescribing them together, and so now, except in rare cases, we use only hydroxychloroquine. We also leave other support devices such as an oximeter, or tanks of oxygen. Above all, we stay in touch with the patients and their families, and monitor the course of treatment on a daily basis.
So far we have visited almost 300 patients. We can do this thanks to the hospital’s resources and private donations of protective equipment. Every time we enter a patient’s home we wear two gowns, two masks, caps, shoe covers. We’re extremely careful. I’m almost embarrassed to say this, but even when I’m at home with my wife, I keep the mask on.
I’m one of those doctors who could have retired, but I chose not to. I’m not an alarmist by nature, but this is a tragedy. And we all need to do what we can, and what we can do best, to deal with it. —As told to Francesca Berardi

Ben Davis, 35, is the program director and a social worker at Center for Urban Community Services in New York
We’re a program at the Center for Urban Community Services (CUCS) working with adults living with serious mental illness. The people in our program, most of whom live in the Bronx, have had multiple psychiatric hospitalizations and have tried getting help from clinics and other mental health programs without long term success. The goal of our program is to help our clients thrive in the community without hospitalization and to reach their life goals. We bring all the services to the people where they are. If they live in a private apartment we see them at home, if they’re homeless we go and see them on the street, or if they are in a shelter we see them there. We provide psychotherapy, psychiatric care, and assistance with medication and other medical issues. We work with their families, address legal issues, go grocery shopping or help them with cleaning, if they’re interested in employment and education—really everything we can to help them reach their goals and maintain wellness in the community.
[With COVID-19] our job is different in almost every way. We are looking at all of the different things that our clients need and how to prioritize them. Which of those can we only provide face-to-face? And which of those can we provide remotely by phone? We try to do video conferencing by phone when we can, but it’s so hard to assess and really know what’s going on with people that way. Some of our folks have difficulty with communication and it has been very anxiety provoking not being able to see them in person. When we think it is critical we go and see them in person because we need to. This particularly includes delivering and administering medication. We take all the precautions we can when we do this.
A lot of the individuals we work with experience paranoia as part of their psychiatric symptoms. What is happening right now feels like their fears are being made real. People who already have a lot of fear of contamination and germs and of other people in general are isolating themselves even more now. In normal times we are there to help them get out more. Now we’re telling them to stay in. We are worried that this necessary isolation might be heightening their paranoia and making it worse.
I just went to see someone this morning. I’m wearing a mask and standing at a distance. When I gave him a phone, so we could be in better touch, I couldn’t just hand it to him for safety. I had to put it on the ground and asked him to pick it up. He was freaked out by that. It was all very different and very confusing. I don’t know how well he understood that I was doing it to help keep him safe.
The dedicated case managers, social workers, physicians, nurses, and administrators on my team have all been so willing to adapt and adjust, they are doing such great work. In less than a week we needed to redesign our entire program and change how we do everything. I’m optimistic that whatever comes, if this stretches for months on end, that we’ll be able to adapt to it and step up. We are thinking long term. We are planning for this to be for months, because we have to. That’s including things like our procedures around wearing masks. If we run out of gloves, we can’t administer medications anymore. Everything we’re doing now is planning for the long term.
The folks that we work with are among the most vulnerable in our society. When society is functioning at its best, they face incredible challenges because of their mental illness, because of trauma history, because of structural inequality, you name it. Every challenge they face in society when everything’s functioning well is heightened now.
But our clients are survivors. They have been through everything, have lived through things I can’t imagine. They are still here and they’re persistent. I believe that they have that mindset that they’ve been able to get through things before and they’ll be able to get through this now. I try to be optimistic that they’ll be okay. We are there no matter what to help them. —As told to Abigail Abrams

Felipe, 53, works at a hog farm in North Carolina
Unfortunately those of us who work in hog farms have to work every day, since the animals need to be fed every day. If we don’t go, there isn’t anyone to feed them. For us, a day worked is a day paid. If we were to miss work because of the pandemic, we will not be paid.
Some of my colleagues are undocumented. My wife, who is also from Mexico, is undocumented and works at a vegetable packing shed.
It doesn’t seem fair to us that immigration reform hasn’t passed because really, we’re the ones who are working. And we’re helping a little bit to make sure the country has, for example, produce and, in our case, meats. So it seems to us a little wrong that they are not helping us for the simple fact that they are undocumented. They’re not helping the people who work.
I’ve talked about this with my colleagues. There are some who are undocumented who are working, and they won’t get anything [help from the government] and they’re doing the work.”

Yolanda Fisher, 48, is a cafeteria worker at T.W. Brown Middle School in Dallas, Texas
I’m still going to work because we’re still feeding the kids—it’s not just kids that attend my school, it’s any child that stayed in Dallas and they need a meal. And if a family is really in need, we give the adults a meal as well. When it first started we would come in from 6:30 in the morning until 5 in the evening, working weekends and stuff, but now it’s leveling off. I’m loving it because I miss [the kids’] faces. You miss hearing their noise. We are feeding our community, and I love that.
I’m very nervous [about contracting the virus]. I have two grandchildren at home, aged 4 and 9. I could harm my family if I bring something home. That’s always in the back of my mind. We have gloves, we wash our hands, we have sanitizers. The mask I have I purchased on my own—the school didn’t have masks. They told us we could tie a bandana around our face, that that would work.
My daughter takes my temperature every day I come home. If she wants to spray me down with Lysol that’s fine, anything to alleviate her fears. My daughter at one point said, ‘Mom you’re older, older people are dying, you can stay home,’ but I was like nah. Jesus was a server. That’s my purpose. That’s why I’ve been in this business 26 years. Most people look at us as a cafeteria lady, I look at it as a service. If there wasn’t an epidemic we would be still serving kids who probably would not get another meal until the next day. It’s an honor for us to serve those kids. —As told to Alana Abramson

Scott Gray, 49, is a client center manager at St. Mary’s Food Bank Alliance in Phoenix, Ariz.
We went from serving 500-600 people per day to, on average, 1,200 a day in the last two weeks. We did 1,500 people yesterday. The days start off with us coming in at 7:00 and the line is already going down the sidewalk with people waiting in line for food. And to see the elderly out there with their carts, and a mom with kids and they are standing in line at 7 in the morning… [I’ve] never seen anything like this. The first thing in my mind is what do we have available? How can I make it stretch?
Donations have increased a lot, it’s by the truckloads. Most people who show up have never been to a food bank, they think we’re a soup kitchen. People are shocked when they realize they are getting a basket to take home of supplies for the whole family. They see the basket and say, “This is all for me?” Not only am I feeding my family by working, but the families that are in line are feeding theirs. It’s an awesome feeling.
I’m worried that this will become the norm, dealing with this many people. Will the food bank become a place we have to shut down because of social distancing? Or because it gets out of control? What are we getting in tomorrow? Will that donation be enough? But right now I don’t see that being a problem for what we’re doing and the way we’re doing it. If I get sick it would have been for a good cause. —As told to Alana Abramson
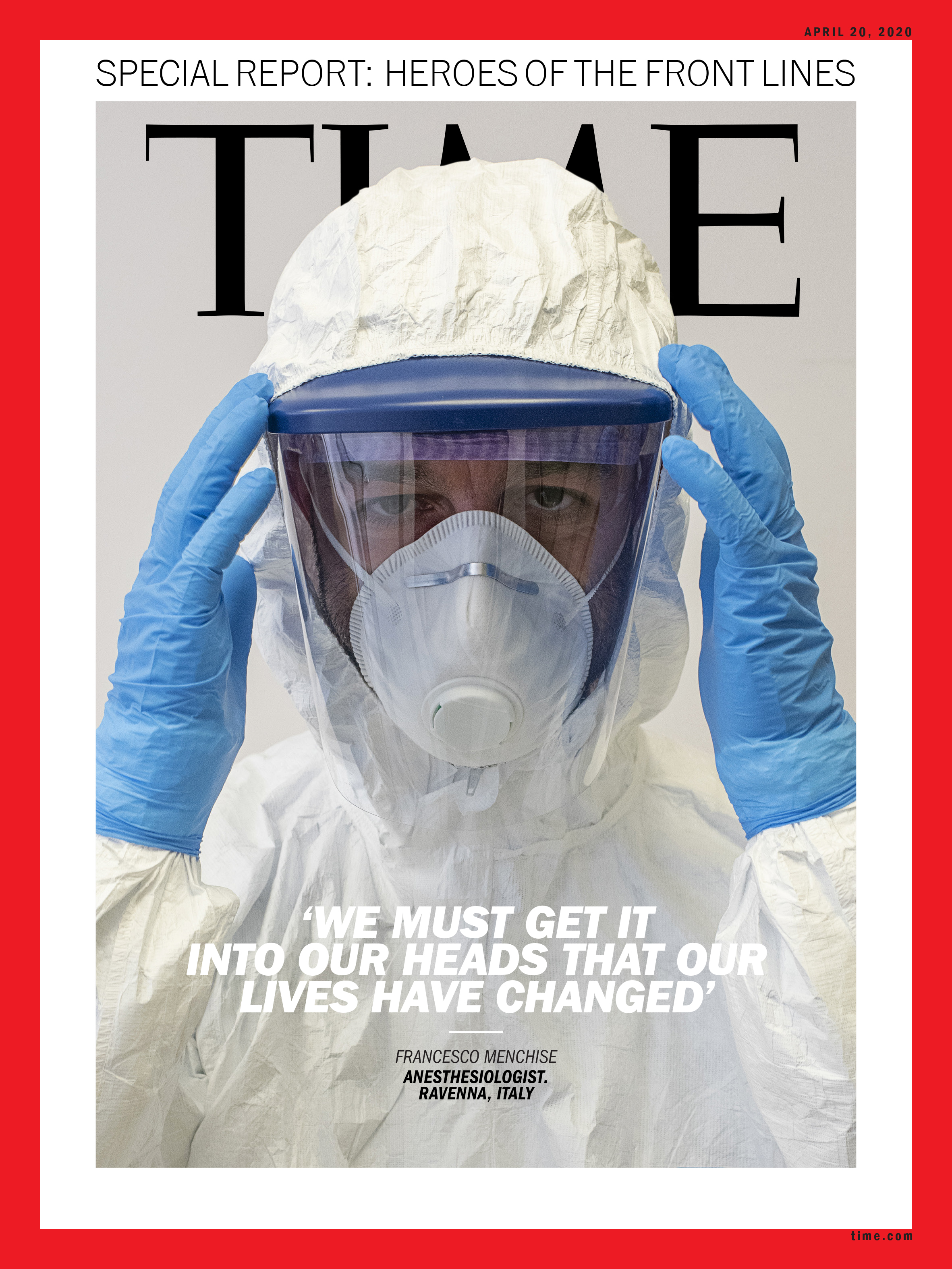
Francesco Menchise, 42, is an anesthesiologist on the COVID-19 intensive care unit at Santa Maria delle Croci hospital in Ravenna, Italy
Intubation operations are those where you are most exposed to the patient’s aerosol. You might sweat inside the protective gear, but it’s necessary. Our team consists of eight people plus a coordinator expert in emergencies and natural disasters. We are used to being under pressure, but we have never been under as much pressure as we are now. There’s been no lack of protective equipment (PPE), but of course we are all afraid of getting infected. Fortunately, so far no one has shown any symptoms.
The most obvious effect of the stress is that I no longer sleep well. I work about the same number of hours as before, 40 a week, but it’s more demanding on a mental level. Our patients remain on the ward for two or three weeks, much longer than on an average before the COVID-19 epidemic. More than 50% of those intubated don’t make it, and one of the most painful aspects of these deaths is that relatives cannot see their loved ones one last time.
My personal therapy is cooking. When I can, I cook. Like all Italians at this moment, those who cooked already cook more, those who didn’t cook have started to. We’ve all become 100% Italian again.
But we will have to roll up our sleeves for a long time. We must get it into our heads that our lives have changed, and until we find a therapy we have to learn to live with this virus. —As told to Francesca Berardi

Matt Monaghan, 47, is a bus driver in New York City
We have a lot of drivers that are out, many have been sick. Some have been able to recover. And as the days go by more and more get sick, and it just gets worse.
My bus was normally crowded, but now, some mornings I get five people in. They sit apart, and the first three rows are chained off to keep us safe. Our cleaners constantly disinfect the buses for us. I carry my own Lysol. My union, the Amalgamated Transit Union, supplied us with gloves and masks. New York City Transit in the beginning did not give us anything, though they have since offered masks.
Luckily, I’m a single guy who lives alone, so I really can’t bring this home to anybody. But we have a lot of drivers here that have families. We have drivers that have their parents living with them who are older. We come to work because we have to keep the city moving, but my anxiety is through the roof.
Unfortunately, you see a lot of people who don’t need to be out. When I’m not working on a bus, I’m home, self quarantining. I was aggravated about it. For them to put up on the busses [signs that say]: “If you have to cough or sneeze, please do it into your elbow.” You shouldn’t have to tell anybody that on a good day, let alone when you’re in the middle of a pandemic. I think the mindset is people think it’s just older people who are getting sick. Everybody’s dying from it. Just take it seriously. —As told to Abby Vesoulis
Dr. Aslam Parvez, 42, and Dr. Sonia Rani Parvez, 41, are physicians in Patiala, India
I, Dr. Aslam Parvez and my wife, Dr. Sonia Rani Parvez, are working as rural medical officers in peripheral rural areas of district Patiala, in Punjab, India. We have been married for 15 years and we have a son, Ayaan, who is 8 years old. Before the pandemic, we could go out to walk, exercise, spend time with our kid, make him study, party or picnic. There was work and targets to meet but we never thought that we would have to work so much on ourselves to remain mentally strong.
These are never before seen times. Everywhere in the world health staff is facing the same set of problems and they need to be motivated all the time. I tell them, “We are warriors and we have to win this war either with or without weapons.”
It was Feb. 10, I remember the date, that it started to affect our jobs and we started mentally preparing [for COVID-19]. Ayaan was having his final exams, starting on Feb. 18, and the day his exams finished, we took him to visit his grandparents by himself. He had not stayed alone there in the past—it’s nearly 60 miles away from our home, and a 1 hour 30 minute drive. There was no pandemic declaration by WHO at the time, but when he left, we were told to have our teams ready by the state government. I volunteered to post myself in a rapid response team, and Sonia volunteered to work in the COVID isolation ward. We were mentally preparing ourselves for this fight for the last month, and figured our child would be safe with his grandparents. With a short training we were ready. It’s very difficult to get excited about these things, but we consider it as an honor to serve our people.
Now, we may not see Ayaan for quite some time. We are not planning to get him till the pandemic is over, and after that, we will take quarantine for two or more weeks. Sonia sometimes gets teary eyed while talking to him but he tells his mom to keep going as he is a busy, brave kid. I miss him too but I know he is safe away from us.

Cliff Strand Jr., 50, is an employee for White Pony Express in Pleasant Hill, Calif.
I’m a product of what White Pony Express does for people. About six years ago, one of our executives found me under a bridge in Richmond, Calif., and brought me baskets of food. I was a strung-out-of-my-mind drug addict with a dark soul, ready to die. He helped me. This is absolutely my mission. It’s not a job. I’m supremely blessed to be able to do this.
Not for a minute did I consider staying home during this outbreak. It takes that level of fear down to show people that we’re out here and taking the right precautions. I change my gloves at every location and wear a mask.
I delivered food to the local shelter, the Contra Costa Interim Housing Shelter, and there’s over 100 people in there. I know those people; they’re my friends. Now they’re behind a wall to prevent the virus from spreading. It brought me to tears. We’re flashing up heart signs and saying, ‘I love you’ through the wall. I was crying, but it wasn’t because there was fear. There’s love going on in this whole thing. —As told to Jamie Ducharme
[White Pony Express collects excess food from restaurants, grocery stores and distributors, and delivers it to people and organizations in need. During the outbreak, they’ve rescued about 17,000 pounds of food per day instead of their usual 7,000.]
- Donald Trump Is TIME's 2024 Person of the Year
- TIME’s Top 10 Photos of 2024
- Why Gen Z Is Drinking Less
- The Best Movies About Cooking
- Why Is Anxiety Worse at Night?
- A Head-to-Toe Guide to Treating Dry Skin
- Why Street Cats Are Taking Over Urban Neighborhoods
- Column: Jimmy Carter’s Global Legacy Was Moral Clarity