There are few things as powerful as avoidance learning. Touch a hot stove once and you’re not likely to do it again. Cross against the light and almost get hit by a car and you’re going to be a lot more careful the next time. But when it comes to the U.S. response to COVID-19? Not so much.
You’d have thought that the sight of overflow hospital tents and refrigerated trucks to hold victims’ bodies in New York would have been enough to scare us all straight in mid-March and early April, when infection rates peaked at 32,000 new cases a day, or nearly 10 cases per 100,000 residents—making social distancing, mask-wearing and hand-washing all universal practices. But shortly after that peak, the warm weather arrived and several states cautiously reopened some public spaces for Memorial Day.
That, as we wrote at the time, quickly led to distressing signs of upticks in several states, pushing the national rate marginally north again. By the end of June, the rolling average of new cases per day had far exceeded the April peak, prompting some states to pull back their reopening plans. But the damage had been done. By mid-July, a second wave peaked at over twice the value of the first, exceeding 67,000 cases per day—more than 20 cases per capita. There was good news buried in that bad news, however: after the peak was reached, the decline was at least quicker and more precipitous than it was the first time.
But now for the worse news: Heading into the fall and winter, there are clear signs of a third resurgence bearing a close resemblance to what we saw in early June. Since the most recent nadir on Sept. 9, when the national rate was at 34,300 cases a day—still a notch above the April peak—cases have risen to 45,300 a day, a 32% increase. The numbers paint an alarmingly familiar picture that spells trouble ahead—despite President Donald Trump’s repeated but false assertions that the country is “rounding the final turn” on the pandemic.
“The latest information is that 90% of the country has not yet been exposed to the virus,” says Dr. Tom Inglesby, director of the Johns Hopkins Center for Health Security at the Bloomberg School of Public Health. “The virus hasn’t changed and has the capacity to spread rapidly if given a chance.”
It’s now getting that chance. The politicization of mask-wearing; conflicting guidelines from the White House, the Centers for Disease Control and Prevention and the Food and Drug Administration; and state and local policies that contribute to viral transmission are helping to do the disease’s work for it.
“A single and coordinated strategy might have brought us to a different place,” says Dr. Jon Samet, dean of the Colorado School of Public Health. “Even within some states, counties may proceed independently. There is wide variation in the credence given to misinformation, some sourced from the Administration and even the President.”
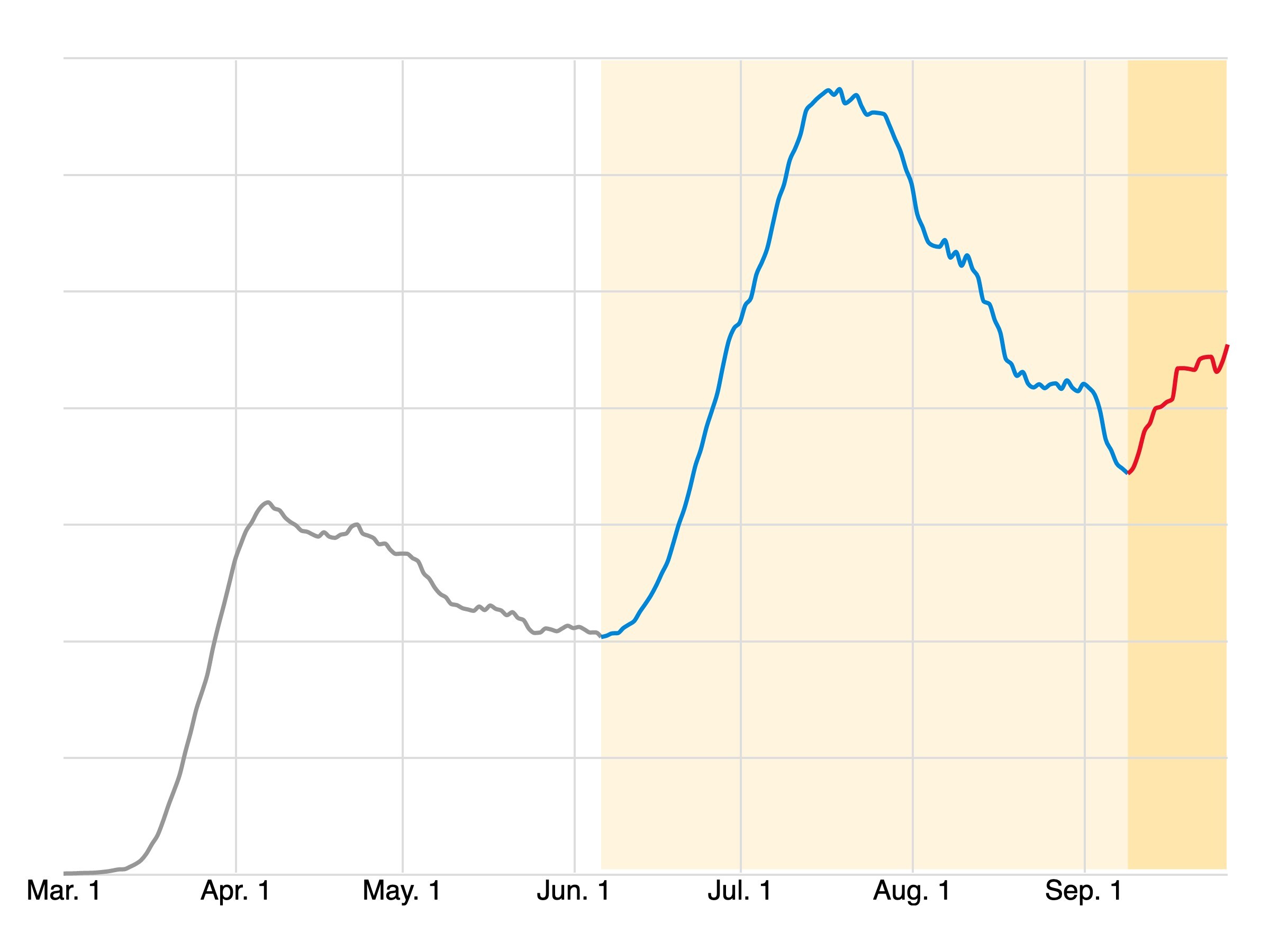
Samet’s own state offers a vivid example of the rise of the third wave, with its graph since spring forming a stark, three-peaked mountain range, not unlike a view you might find while hiking in the Colorado Rockies:
In some ways, however, Colorado is an outlier in the new wave—or at least lies at its very vanguard. The first wave hit hardest in the Northeast; the second in the South and the West. Now, even as cases balloon in the South again (driven in large part by Texas and Florida), the Midwest has surpassed the West in cases, with dramatic spikes from Wisconsin and Minnesota to the Dakotas and down to Utah and Wyoming:
At a more granular level, the geographic trends become even clearer. There are more than 3,000 counties (or county-equivalents, like parishes) in the U.S., almost all of which report individual daily figures for new COVID-19 positive tests. Breaking them down into three categories—small, medium and large, each with about a third of the U.S. population—reveals that the 62 largest counties, which are home to 110 million people, were responsible for more cases than either of the other two categories through mid-August. Now the story has flipped, with the bloc of smallest counties—encompassing the same number of total people but distributed across a much larger, more rural geography—contributing the most new cases:
“Given that these are rural areas, behaviors of individuals are likely to be a dominant driver: not adhering to distancing and not wearing masks,” says Samet. “Checking across mask orders in these states, there is a wide range. I suspect adherence to use of masks is lower in these rural counties than in urban areas, as in Colorado by anecdotal reports.”
There has also been a shift in COVID-19 age demographics that in turn affect the regional situation. “In part of the Midwest, the rise is being driven by young adults who seem to have gotten the coronavirus in universities,” says Inglesby. It doesn’t help that college students—who are by nature less risk-averse than older people—are being enabled in their heedlessness by a lack of guidance from adults who ought to know better. It’s also worth noting that many young Americans hold jobs that increase exposure risk, like retail or restaurant work.
Whatever the manifold causes of the third wave, there is reason to worry that it will prove worse than the first two. The arrival of colder weather in some states means more time spent indoors, where viruses are more easily transmitted by aerosols produced when people sneeze, cough or merely speak. With the pandemic still raging, many people will likely scrap seasonal travel and family get-togethers for Thanksgiving, Christmas and so on—but many are likely to press ahead regardless, meaning minimal social distancing in crowded planes and trains and around holiday dinner tables.
“We are concerned that there could be a holiday spike with severity depending on where the epidemic curve is positioned before the start of the season in later November,” says Samet.
Whether the third wave will be followed by a fourth is, paradoxically, both impossible to say and entirely within our control. Hopefully, greater policy coherence from Washington, uniform national rules around masking and distancing, and broad public acceptance of an eventual vaccine—once it is proven to be safe and effective—will all, at last, stuff the COVID-19 genie back into its bottle. Until then, the U.S., which represents only 4% of the world’s population yet has reported more than 20% of its COVID-9 cases and deaths, will continue to struggle. It is up to all of us, working together, to bring that suffering to an end.
More Must-Reads from TIME
- Why Trump’s Message Worked on Latino Men
- What Trump’s Win Could Mean for Housing
- The 100 Must-Read Books of 2024
- Sleep Doctors Share the 1 Tip That’s Changed Their Lives
- Column: Let’s Bring Back Romance
- What It’s Like to Have Long COVID As a Kid
- FX’s Say Nothing Is the Must-Watch Political Thriller of 2024
- Merle Bombardieri Is Helping People Make the Baby Decision
Write to Chris Wilson at chris.wilson@time.com and Jeffrey Kluger at jeffrey.kluger@time.com