
It wasn’t greed, or curiosity, that made Li Rusheng grab his shotgun and enter Shitou Cave. It was about survival. During Mao-era collectivization of the early 1970s, food was so scarce in the emerald valleys of southwestern China’s Yunnan province that farmers like Li could expect to eat meat only once a year–if they were lucky. So, craving protein, Li and his friends would sneak into the cave to hunt the creatures they could hear squeaking and fluttering inside: bats.
Li would creep into the gloom and fire blindly at the vaulted ceiling, picking up any quarry that fell to the ground, while his companions held nets over the mouth of the cave to snare fleeing bats. They cooked them in the traditional manner of Yunnan’s ethnic Yi people: boiled to remove hair and skin, gutted and fried. “They’d be small ones, fat ones,” says Li, now 81, sitting on a wall overlooking fields of tobacco seedlings. “The meat is very tender. But I’ve not been in that cave for over 30 years now,” he adds, shaking his head wistfully. “They were very hard times.”
China today bears little resemblance to the impoverished nation of Li’s youth. Since Deng Xiaoping embraced market reforms in 1979, the Middle Kingdom has gone from strength to strength. Today it is the world’s No. 2 economy and top trading nation. It has more billionaires than the U.S. and more high-speed rail than the rest of the world combined. Under current strongman President Xi Jinping, China has embarked on a campaign to regain “center place in the world.” Farmers like Li no longer have to hunt bats to survive.
That doesn’t mean Shitou Cave has faded in significance. Today, though, its musty depths speak not to local sustenance but global peril. Shitou was where Shi Zhengli, lead scientist at the Wuhan Institute of Virology (WIV), working with samples of bat feces in 2011 and 2012, isolated a novel virus that was very similar to SARS, which had been responsible for a pandemic a decade earlier. Shi–known as China’s “bat woman” for her tireless research on the winged mammal–warned that other bat-borne diseases could easily spill over into human populations again. Seven years later, her fears appear vindicated. In a February paper, Shi revealed the discovery of what she called the “closest relative” of what would become known as SARS-CoV-2, the coronavirus that causes COVID-19. It also originated in a bat colony just 90 miles from Shitou Cave.
Dubbed RaTG13, Shi’s virus has a 96.2% similarity with the virus that has claimed some 600,000 lives across the world, including more than 140,000 in the U.S. Shi’s discovery indicates COVID-19 likely originated in bats–as do rabies, Ebola, SARS, MERS, Nipah and many other deadly viruses.
But how did this virus travel from a bat colony to the city of Wuhan, where the coronavirus outbreak was first documented? And from there, how did it silently creep along motorways and flight routes to kill nurses in Italy, farmers in Brazil, retirees in Seattle? How this virus entered the human population to wreak such a devastating toll is the foremost issue of global scientific concern today. The search for “patient zero”–or the “index case,” the first human COVID-19 infection–matters. Not because any fault or blame lies with this individual, but because discovering how the pathogen entered the human population, and tracing how it flourished, will help the science and public-health communities better understand the pandemic and how to prevent similar or worse ones in the future.
On top of the millions of lives that hang in the balance, Cambridge University puts at $82 trillion across five years the cost to the global economy of the current pandemic. The human race can ill afford another.
The provenance of COVID-19 is not only a scientific question. The Trump Administration also regards it as a political cudgel against Beijing. As the U.S. has failed to control outbreaks of the coronavirus and its economy founders, President Donald Trump has deflected blame onto China.
Trump and senior Administration figures have dubbed COVID-19 the “China virus” and “Wuhan virus.” Secretary of State Mike Pompeo said there was “enormous evidence” the virus had escaped from Shi’s lab in the city. (He has yet to share any hard evidence.) “This is the worst attack we’ve ever had on our country. This is worse than Pearl Harbor. This is worse than the World Trade Center,” Trump said in May of the pandemic, pointing the finger at China. In response, Chinese Foreign Minister Wang Yi accused the U.S. President of trying to foment a “new cold war” through “lies and conspiracy theories.”
The origin of the virus is clearly a touchy subject. Nevertheless, the world desperately needs it broached. Australia and the E.U. have joined Washington’s calls for a thorough investigation into the cause of the outbreak. On May 18, Xi responded to pressure to express support for “global research by scientists on the source and transmission routes of the virus” overseen by the World Health Organization.
But Trump has already accused the WHO of being “Chinacentric” and vowed to stop funding it. His attacks may have some basis in fact. The organization refused self-governing Taiwan observer status under pressure from Beijing. And privately, WHO officials were frustrated by the slow release of information from the Chinese authorities even as they publicly praised their transparency, according to transcripts obtained by the Associated Press.
Partisan bickering and nationalism threaten to eclipse the invaluable scientific work required to find the true source of the virus. Time is of the essence; a SARS vaccine was within touching distance when research that could have proved invaluable today was discontinued as the crisis abated. “Once this pandemic settles down, we’re going to have a small window of opportunity to put in place infrastructure to prevent it from ever happening again,” says Dr. Maureen Miller, a Columbia University epidemiologist.
The search for the virus’s origins must begin behind the squat blue-shuttered stalls at Wuhan’s Huanan seafood market, where the outbreak of viral pneumonia we now know as COVID-19 was first discovered in mid-December. One of the first cases was a trader named Wei Guixian, 57, who worked in the market every day, selling shrimp out of huge buckets. In mid-December she developed a fever she thought was a seasonal flu, she told state-run Shanghai-based the Paper. A week later, she was drifting in and out of consciousness in a hospital ward.
Of the first 41 patients hospitalized in Wuhan, 13 had no connection to the marketplace, including the very first recorded case. That doesn’t necessarily excuse the market as the initial point of zoonotic jump, though–we don’t know yet for certain how many COVID-19 cases are asymptomatic, but research suggests it could be as high as 80%. And, even if Huanan market wasn’t where the virus first infected humans, it certainly played a huge role as an incubator of transmission. At a Jan. 26 press conference, the Hong Kong Centre for Health Protection revealed 33 of 585 environmental samples taken after the market was shut Jan. 1 tested positive for the virus. Of these, 31 were taken in the western section where wildlife was sold.
In May, China acceded to demands for an independent inquiry after more than 100 countries supported a resolution drafted by the E.U. Still, President Xi insists it must be “comprehensive”–looking not just at China but also at how other nations responded to the WHO’s warnings–and cannot begin until after the pandemic has subsided. “The principles of objectivity and fairness need to be upheld,” Xi told the World Health Assembly. (Notably, inquiries into the 2009 H1N1 “swine flu” pandemic and 2014 West African Ebola outbreak began before the crises had abated.) According to past investigations’ protocols, teams are composed of independent public-health experts and former WHO staff appointed by the WHO based on member states’ recommendations. At a practical level, however, any probe within China relies on cooperation from Beijing, and it’s uncertain whether the U.S. will accept the findings of a body Trump has slammed for “severely mismanaging and covering up the spread of the coronavirus.”
Peter Ben Embarek, a food-safety and animal-disease expert at the WHO, says an investigation must concentrate on interviews with all the initial cases, trying to find clues about potential earlier infections among their relatives, their contacts, and where they had been over the days and weeks before they got sick. Also, which hunters and farmers supplied what species of animals. “With a bit of luck and good epidemiological work, it can be done,” he says.
There are many who look at where COVID-19 emerged and see something that can’t be just a co-incidence. In 2017, China minted its first biosecurity-level 4 (bsl-4) laboratory–the highest level cleared to even work with airborne pathogens that have no known vaccines–in Wuhan. Ever since, the country’s foremost expert on bat viruses has been toiling away inside the boxy gray buildings of the WIV. Indeed, when Shi first heard about the outbreak, she herself thought, “Could they have come from our lab?” she recently told Scientific American. An inventory of virus samples reassured her that it hadn’t, she added, yet that hasn’t stopped some from maintaining their suspicions.
Mistakes do happen. The last known case of small-pox leaked from a U.K. laboratory in 1978. SARS has leaked from Chinese laboratories on at least two occasions, while U.S. scientists have been responsible for mishandlings of various pathogens, including Ebola. There are only around 70 bsl-4 laboratories in 30 countries. Suspicions regarding the nature of research under way inside the Wuhan laboratory persist. According to one leading virologist, who asked to remain anonymous for fear of jeopardizing funding and professional relationships, “Were you to ask me where’s the most likely place in the world for a naturally occurring bat coronavirus to escape from a laboratory, Wuhan would be in the top 10.”
Still, neither the WHO nor the Five Eyes intelligence network–comprising the U.S., U.K., Canada, Australia and New Zealand–has found evidence that COVID-19 originated from Shi’s lab. Canberra has even distanced itself from a U.S.-authored dossier that sought to convince the Australian public that the Five Eyes network had intelligence of a Chinese cover-up. (It appeared to rely exclusively on open-source material.) Meanwhile, scientific peers have rallied to defend Shi from suspicion. “She is everything a senior scientist should be,” says Miller, who has collaborated with Shi on various studies. The Wuhan Institute of Virology did not respond to requests for comment.
Available evidence suggests COVID-19 leaped from wild animal to human. Tracing exactly how is crucial. It enables governments to install safeguards regarding animal husbandry and butchery to prevent any repeat. SARS, for example, originated in bats and then infected a palm civet, a catlike mammal native to South and Southeast Asia. The animal was then sold at a wet market–where fresh meat, fish and sometimes live animals are sold–in Guangdong, from which it jumped to humans. In the wake of that outbreak, which claimed at least 774 lives worldwide, palm civets were banned from sale or consumption in China. Bats may have been the initial reservoir for SARS-CoV-2, but it’s likely that there was an intermediary before it got to humans, and that’s where the possibilities grow. Bats share Shitou Cave with starlings, for one, and at least one large white owl nests in its upper reaches. Herds of black and white goats graze the dusty shrub all around the cave opening, while the Yi ethnic group traditionally rear and eat dogs. Bat guano is also traditionally prized as a fertilizer on crops.
Just a few miles from Shitou, customers at Baofeng Horse Meat restaurant squat by round tables, slurping green tea poured from enormous brass teapots, while charcoal burners cook up the eponymous cuts alongside dogmeat and other specialties. “All the animals we sell are reared nearby,” says proprietor Wang Tao. Cultural practices and disease-transmission vectors are often entwined. MERS continues to jump between camels and their human handlers on the Arabian Peninsula. China’s penchant for eating rare and unusual wildlife for obscure health benefits may have contributed to the current pandemic. While many aspects of Traditional Chinese Medicine (TCM) are entirely benign, involving little more than massage, pressure points and bitter herbs, there is a fetishization of exotic animals, and there’s some evidence that TCM might have played a role in launching the pandemic. The receptor-binding domain of SARS-CoV-2’s spike protein–which the virus uses to bind to hosts–is unusually adept at attaching to human cells. New viruses discovered in Malaysian pangolins have since been shown to have exactly the same receptor binders. “Some features in [SARS-CoV-2] that initially may have looked unusual, you’re now finding in nature,” says Edward Holmes, an evolutionary biologist and virologist at the University of Sydney.
That COVID-19 originated in bats and then jumped to humans via a pangolin intermediary is now the most likely hypothesis, according to multiple studies (although some virologists disagree). Up to 2.7 million of the scaly mammals have been plucked from the wild across Asia and Africa for consumption mostly in China, where many people believe their scales can treat everything from rheumatoid arthritis to inflammation. Their meat is also highly prized for its supposed health benefits.
On Feb. 24, China announced a permanent ban on wildlife consumption and trade, scratching out an industry that employs 14 million people and is worth $74 billion, according to a 2017 report commissioned by the Chinese Academy of Engineering. It’s again extremely sensitive. President Xi is an ardent supporter of TCM and has promoted its use globally. The total value of China’s TCM industry was expected to reach $420 billion by the end of this year, according to a 2016 white paper by China’s State Council. And rather than raising the possibility that misuse of TCM sparked the outbreak, Chinese state media has lauded–without evidence–the “critical role” TCM has played in the treatment of COVID-19 patients. In an apparent attempt to head off criticism related to the pandemic, draft legislation was published in late May to ban any individual or organization from “defaming” or “making false or exaggerated claims” about TCM. Cracking down on the illicit animal trade would go a long way toward preventing future outbreaks. But as demand for meat grows across increasingly affluent Asia, Africa and Latin America, the potential for viruses to spill over into human populations will only increase.
It probably wasn’t blind luck that Li and his friends didn’t get sick from their hunting expeditions in Shitou Cave. Research by Columbia’s Miller with WIV’s Shi, published in 2017, found that local people were naturally resistant to SARS-like viruses. Examining their lifestyle habits and antibodies can help deduce both mitigating factors and possible therapies, while pinpointing which viruses are particularly prone to infecting humans, potentially allowing scientists to design vaccines in advance. “They are the canaries in the coal mine,” says Miller.
The cloud of uncertainty surrounding the virus’s origins may never lift. Identifying an individual “patient zero” where the virus made the jump from animal to human may be rendered impossible by its remarkable ability to spread while asymptomatic. But just as important is uncovering the broader map of how the virus spread and changed genetically as it did so. In theory, that sort of genetic surveillance could foster the development of broad-spectrum vaccines and antivirals that may prove effective against future novel outbreaks. Studying the anatomy of viruses that readily jump between species may even help predict where the next pandemic is coming from, and prepare us for the inevitable next time. So did those of his 40-member team of infectious-disease emergency responders at Providence Regional Medical Center in Everett, Wash. The first time, the alert was part of a routine monthly test. This time, it was the real thing.
Around 9 p.m. on Jan. 20, Dr. George Diaz’s pager rang for the second time that day. So did those of his 40-member team of infectious-disease emergency responders at Providence Regional Medical Center in Everett, Wash. The first time, the alert was part of a routine monthly test. This time, it was the real thing.
The page signaled the first confirmed U.S. case of COVID-19. The patient was a Washington State resident who had recently returned from visiting family in Wuhan, where the disease was spreading rapidly. Aware of his higher risk, and concerned when he developed a fever, the 35-year-old (who wishes to remain anonymous) visited an urgent-care center where he told health care providers about his travel history. They notified the state health department, which in turn helped the care center send a sample for testing to the Centers for Disease Control and Prevention (CDC) in Atlanta–at the time, the only labs running COVID-19 tests. When the test was positive, CDC scientists recommended the patient be hospitalized for observation. And Diaz’s team was paged.
A trained ambulance team arrived at the man’s home, moved him into a specially designed mobile isolation unit, and drove 20 minutes to Providence Regional. There, the patient couldn’t see who greeted him; everyone assigned to his care was garbed in layers of personal protective equipment. Once in his room, he spoke to medical staff only through a tele-health robot equipped with a screen that displayed their faces, transmitted from just outside the room.
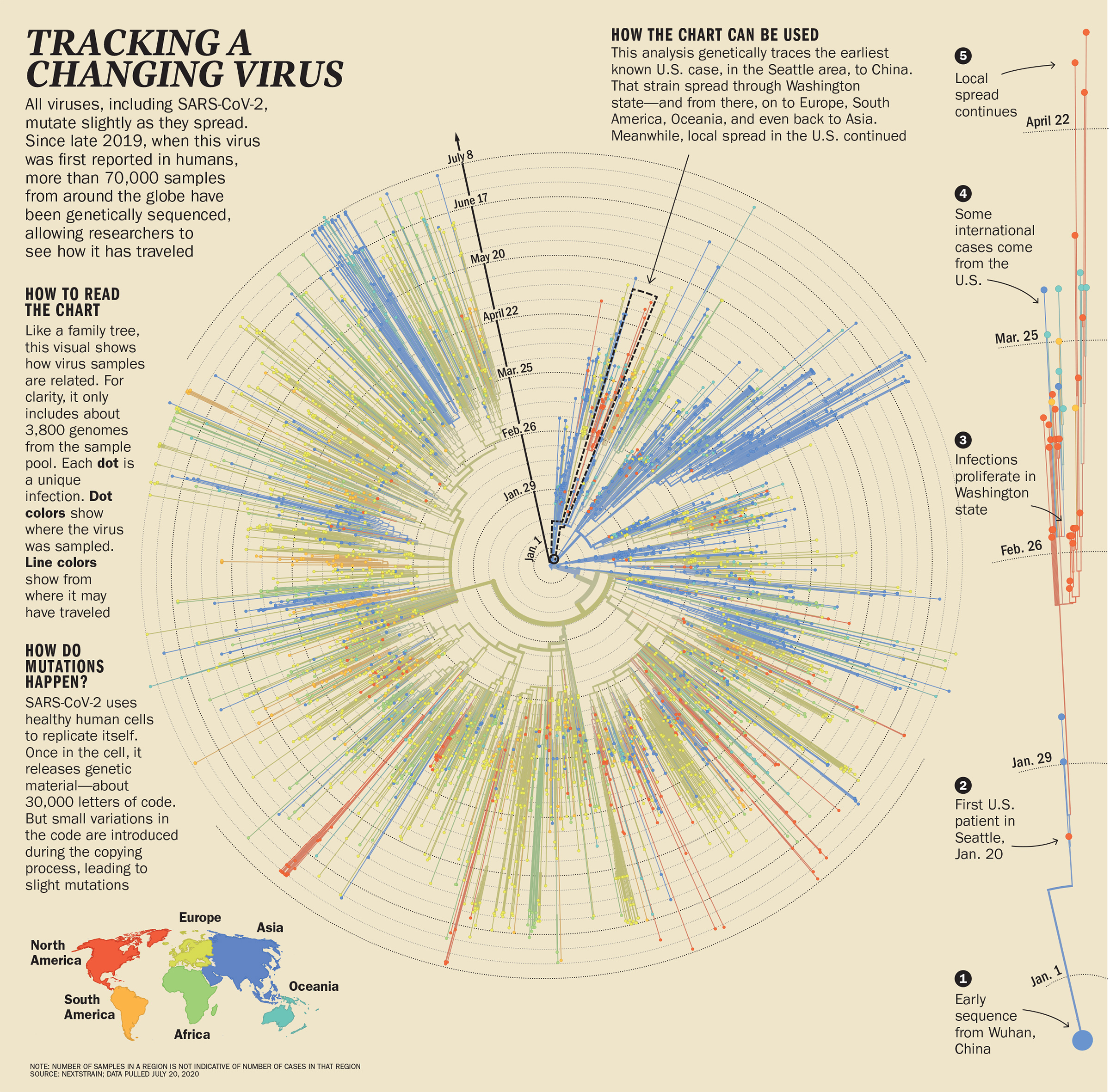
A nurse carefully swabbed the back of his nose and pharynx for a sample of the virus that had brought him to the hospital. Not only was he the first confirmed case of COVID-19 in the U.S., he was also the first in the country to have his virus genetically sequenced. As the index patient in the U.S., his sequence, named WA1 (Washington 1), served as the seed from which experts would ultimately trace the genetic tree describing SARS-CoV-2’s path from person to person across communities, countries and the globe, as it mutated and either died out or moved on with renewed vigor to infect more people.
Genetic sequencing is a powerful tool to combat viruses’ fondness for mutating. Viruses are exploitative and unscrupulous; they don’t even bother investing in any of their own machinery to reproduce. Instead, they rely on host cells to do that–but it comes at a price. This copying process is sloppy, and often leads to mistakes, or mutations. But viruses can sometimes take advantage of even that; some mutations can by chance make the virus more effective at spreading undetected from host to host. SARS-CoV-2 seems to have landed on at least one such suite of genetic changes, since those infected can spread the virus even if they don’t have any symptoms.
Figuring out how to map those changes is a fairly new science. Following the 2014 West African outbreak of Ebola, scientists mapped the genomes of about 1,600 virus samples, collected from the start of the outbreak and representing about 5% of total cases. The work offered insights into how Ebola moved between locations and mutated. But it wasn’t published until 2017, because the majority of the sequencing and sharing of that data was done after the disease’s peak, says Trevor Bedford, associate professor at the Fred Hutchinson Cancer Research Center and co-founder of Nextstrain.org, an open-source database of SARS-CoV-2 genetic sequences. With COVID-19, “everything is happening much more quickly,” he says, which makes the information more immediately useful.
Since the first SARS-CoV-2 genome was published and made publicly available online in January, scientists have mapped the genomes of over 70,000 (and counting) samples of the virus, from patients in China, the U.S., the E.U., Brazil and South Africa, among others. They deposited those sequences into the Global Initiative on Sharing All Influenza Data (GISAID), a publicly available genetic database created in 2008 initially to store and share influenza genomes. During the coronavirus pandemic, it has quickly pivoted to become a clearinghouse for tracking the genetics of SARS-CoV-2, enabling scientists to map the virus’s march across continents and detail its multipronged attack on the world.
“We have genomes from researchers and public-health labs from all over the world on six continents,” says Joel Wertheim, associate professor of medicine at University of California, San Diego. “It provides us with unique insight and confidence that other types of epidemiological data just cannot supply.” Relying on the GISAID sequences, Nextstrain has become a virtual watering hole for scientists–and increasingly public-health officials–who want to view trends and patterns in the virus’s genetic changes that can help inform decisions about how to manage infections.
If genetic sequencing is the new language for managing infectious-disease outbreaks, then the mutations that viruses generate are its alphabet. If paired with information on how infected patients fare in terms of their symptoms and the severity of their illness, genomic surveillance could reveal useful clues about which strains of virus are linked to more severe disease. It might shed light on the mystery of why certain victims of the virus are spared lengthy hospital stays and life-threatening illness. As nations start to reopen, and before a vaccine is widely available, such genetic intel could help health care providers to better plan for when and where they will need intensive-care facilities to treat new cases in their community.
Genetic information is also critical to developing the most effective drugs and vaccines. Knowing the sequence of SARS-CoV-2 enabled Moderna Thera-peutics to produce a shot ready for human testing in record time: just two months from when the genetic sequence of SARS-CoV-2 was first posted. Even after a vaccine is approved and distributed, continuing to track genetic changes in SARS-CoV-2 to ensure it’s not mutating to resist vaccine-induced immunity will be critical. The data collected by Nextstrain will be crucial to help vaccine researchers tackle mutations, potentially for years to come. Already, the group advises the WHO on the best genetic targets for the annual flu shot, and it plans to do the same for COVID-19. “We can track the areas of the virus targeted by the vaccine, and check the mutations,” says Emma Hodcroft from the University of Basel, who co-developed Nextstrain. “We can predict how disruptive those mutations are to the vaccine or not and tell whether the vaccines need an update.”
Meanwhile, genetic surveillance provides real-time data on where the virus is going and how it’s changing. “This is the first time during an outbreak that lots of different researchers and institutes are sharing sequencing data,” says Barbara Bartolini, a virologist at the Lazzaro Spallanzani National Institute for Infectious Diseases in Rome, who has sequenced dozens of viral samples from patients in Italy. That information is giving public-health experts more precise information on the whereabouts of its viral enemy that no traditional disease-tracking method can supply.
After Diaz’s patient tested positive for SARS-CoV-2, Washington State public-health officials diligently traced the places the patient had been and the people he’d come in contact with. He had taken a ride-share from the airport, gone to work and enjoyed lunch at a seafood restaurant near his office with colleagues. But because so little was known about the virus at the time, these contact tracers were focusing mostly on people with symptoms of illness–and at the time, none of the patient’s contacts reported them. The genetics, however, told a different story.
Seattle happened to have launched a program in 2018 to track flu cases by collecting samples from patients in hospitals and doctors’ offices, sites on college campuses, homeless shelters, the city’s major international airport and even from volunteers with symptoms who agreed to swab their nasal passages at home. Those that were positive for influenza and other respiratory illnesses had their samples genetically sequenced to trace the diseases’ spread in the community. As COVID-19 began to emerge in the Seattle area at the end of February, Bedford and his colleagues began testing samples collected in this program for SARS-CoV-2, regardless of whether people reported symptoms or travel to China, then the world’s hot spot for the virus. That’s how they found WA2, the first case in Washington that wasn’t travel-related. By comparing samples from WA1, WA2 and other COVID-19 cases, they figured out that SARS-CoV-2 was circulating widely in the community in February.
If that community-based sequencing work had been conducted earlier, there’s a good chance it might have picked up cases of COVID-19 that traditional disease-tracking methods, which at the time focused only on travel history and symptoms, missed. That would have helped officials make decisions about a lockdown sooner, and might have helped to limit spread of the virus. SARS-CoV-2 moves quickly but mutates relatively slowly, for a virus–generating only about two mutations every month in its genome. For drug and vaccine developers, it means the virus can still evade new treatments designed to hobble it. Those same changes serve as passport stamps for its global trek through the world’s population, laying out the itinerary of the virus’s journey for geneticists like Bedford. The cases in the initial Seattle cluster, he says, appear to have all been connected, through a single introduction directly from China to the U.S. in mid- to late January. Until the end of February, most instances of SARS-CoV-2 in the U.S. piggybacked on unwitting travelers from China. But as the pandemic continued, that changed.
Genetic analysis confirmed that on Feb. 26, SARS-CoV-2 had already hit a new milestone, with the first documented case that it had successfully jumped to a new host in Santa Clara, Calif., one with no travel history to the infectious-disease hot spots in China or known contact with anyone who had traveled there. It’s not clear how this person got infected, but genetic sequencing showed this patient passed on the virus to two health care workers while being treated in the hospital–and that the virus was already spreading in the community, without help from imported cases.
Bedford’s team began to see mutations in samples from Seattle that matched samples from people in Europe and the U.S.’s East Coast. “At the beginning we could kind of draw a direct line from viruses circulating in China to viruses circulating in the Seattle area,” says Bedford. “Later, we see that viruses collected from China have some mutations that were seen later in Europe, and those same mutations were seen in viruses in New York. So, we can draw another line from China to Europe to New York” and then on to Seattle. The virus had begun multiple assaults into the U.S.
Around the world, virologists were seeing similar stories written in the genes of SARS-CoV-2. In January, a couple from Hubei province arrived in Rome, eager to take in the sights of the historic European city. By Jan. 29, they were hospitalized at Lazzaro Spallanzani National Institute for Infectious Diseases with fever and difficulty breathing. Tests confirmed they were positive for SARS-CoV-2.
Bartolini, a virologist at the hospital, and her colleagues compared the genetic sequences from a sample taken from the wife to sequences posted on GISAID. The Italian researchers found it matched five other samples from patients as far-flung as France, Taiwan, the U.S. and Australia. SARS-CoV-2 was clearly already on a whirlwind tour of the planet.
Not all strains of SARS-CoV-2 are equally virulent; some branches of its genetic tree are likely to grow larger and sprout further offshoots, while others terminate more quickly, says Harm van Bakel, assistant professor of genetics and genomic sciences at the Icahn School of Medicine at Mount Sinai. His team conducted the first genetic sequencing analysis of cases in New York City, which quickly became a U.S. hot spot; by March the city had seen a half a dozen or so separate introductions of SARS-CoV-2, but only two resulted in massive spread of the virus. The remainder petered out without transmitting widely.
Retrospectively, there’s no way to tell for sure if these two strains were simply in the right place at the right time–in a particularly densely populated area of the city, for example, or in an area where people congregated and then dispersed to other parts of the city–or if they were actually more infectious. But determining the genetic code of a circulating virus early may help scientists and governments decide which strains are worth worrying about and which aren’t.
From analyzing genetic sequences from 36 samples of patients in Northern California, Dr. Charles Chiu, professor of laboratory medicine and infectious diseases at the University of California, San Francisco, says it might have been possible to identify the major circulating strains and track how they spread if more testing were available to know who was infected–and use this information to guide quarantine and containment practices. “There was a window of opportunity that if we had more testing and more contact-tracing capacities available early on, we likely would have prevented the virus from gaining a foothold at least in California,” he says.
There were similar missed opportunities in Chicago, where genetic sequencing of 88 viruses revealed that the outbreak resulted from three main strains. One was similar to those circulating in New York; one was closely related to the Washington cases and a third never spread appreciably outside the Chicago area. This suggests that stricter travel restrictions might have helped limit introduction of the virus and transmission in northern Illinois.
Ongoing genetic sequencing can also help officials tailor narrower strategies to quell the spread of a virus. It wasn’t long after Beijing reopened following two months of lockdown that infections began creeping up again in June. Sequencing of the new cases revealed that the viruses circulating at the time shared similarities with viruses found in patients in Europe, suggesting the cases were new introductions of SARS-CoV-2 and not lingering virus from the original outbreak. That helped the Chinese government decide to implement only limited lockdowns and testing of people in specific apartment blocks around a food market where the cluster of cases emerged, rather than resort to a citywide quarantine.
And there are other, less obvious ways that genetic analysis of SARS-CoV-2 could help to predict surges in cases as people emerge from lockdown. Italian scientists have sampled wastewater from sewage treatment plants in northern cities where the pandemic flourished, and found evidence of SARS-CoV-2 weeks before the first cases showed up to flood the hospitals. In La Crosse, Wis., Paraic Kenny, director of the Kabara Cancer Research Institute of the Gundersen Health System, applied the same strategy in his hometown in the spring. A few weeks later, in mid-June, when cases of COVID-19 surged because of bars reopening in downtown La Crosse, Kenny compared samples from infected people with the viral genomes in his wastewater samples. They were a genetic match. The same strain of SARS-CoV-2 had been circulating in the community weeks before the cases were reported. “In principle, an approach like this can be used to not just ascertain how much virus is in the community, but maybe give hospitals and public-health departments a warning of when to anticipate a surge in cases,” he says. The goal is to know not just where we are today but where we will be a week or two from now.
It has been 100 years since an infectious disease pushed the entire world’s population into hiding to the extent that COVID-19 has. And the primary approaches we take to combatting emerging microbes today are likewise centuries old: quarantine, hygiene and social distancing. We may never learn exactly where SARS-CoV-2 came from, and it’s clearly too late to prevent it from becoming a global tragedy. But extraordinary advances in scientific knowledge have given us new tools, like genetic sequencing, for a more comprehensive understanding of this virus than anyone could have imagined even a decade or two ago. These are already providing clues about how emerging viruses like SARS-CoV-2 operate and, most important, how they can be thwarted with more effective drugs and vaccines.
This knowledge can save millions of lives–as long as science leads over politics. As unprecedented as this pandemic seems, in both scope and speed, it shouldn’t have caught the world by surprise. For decades, scientific experts have been warning that emerging zoonotic viruses are a threat to humanity of the greatest magnitude. “People keep using the term unprecedented. I’ll tell you, biologically, there is nothing unprecedented about this virus really,” says Holmes, the evolutionary biologist. “It’s behaving exactly as I would expect a respiratory virus to behave.” It’s simply how viruses work, have always worked and will continue to work. The sooner we accept that, the sooner we can act on that knowledge to control outbreaks more quickly and efficiently.
–With reporting by Jamie Ducharme/New York, Madeline Roache/London and John Walcott/Washington
Update: This story has revised the location where RaTG13 was discovered according to newly available information.
More Must-Reads from TIME
- Where Trump 2.0 Will Differ From 1.0
- How Elon Musk Became a Kingmaker
- The Power—And Limits—of Peer Support
- The 100 Must-Read Books of 2024
- Column: If Optimism Feels Ridiculous Now, Try Hope
- The Future of Climate Action Is Trade Policy
- FX’s Say Nothing Is the Must-Watch Political Thriller of 2024
- Merle Bombardieri Is Helping People Make the Baby Decision
Write to Charlie Campbell/Yuxi, Yunnan at charlie.campbell@time.com