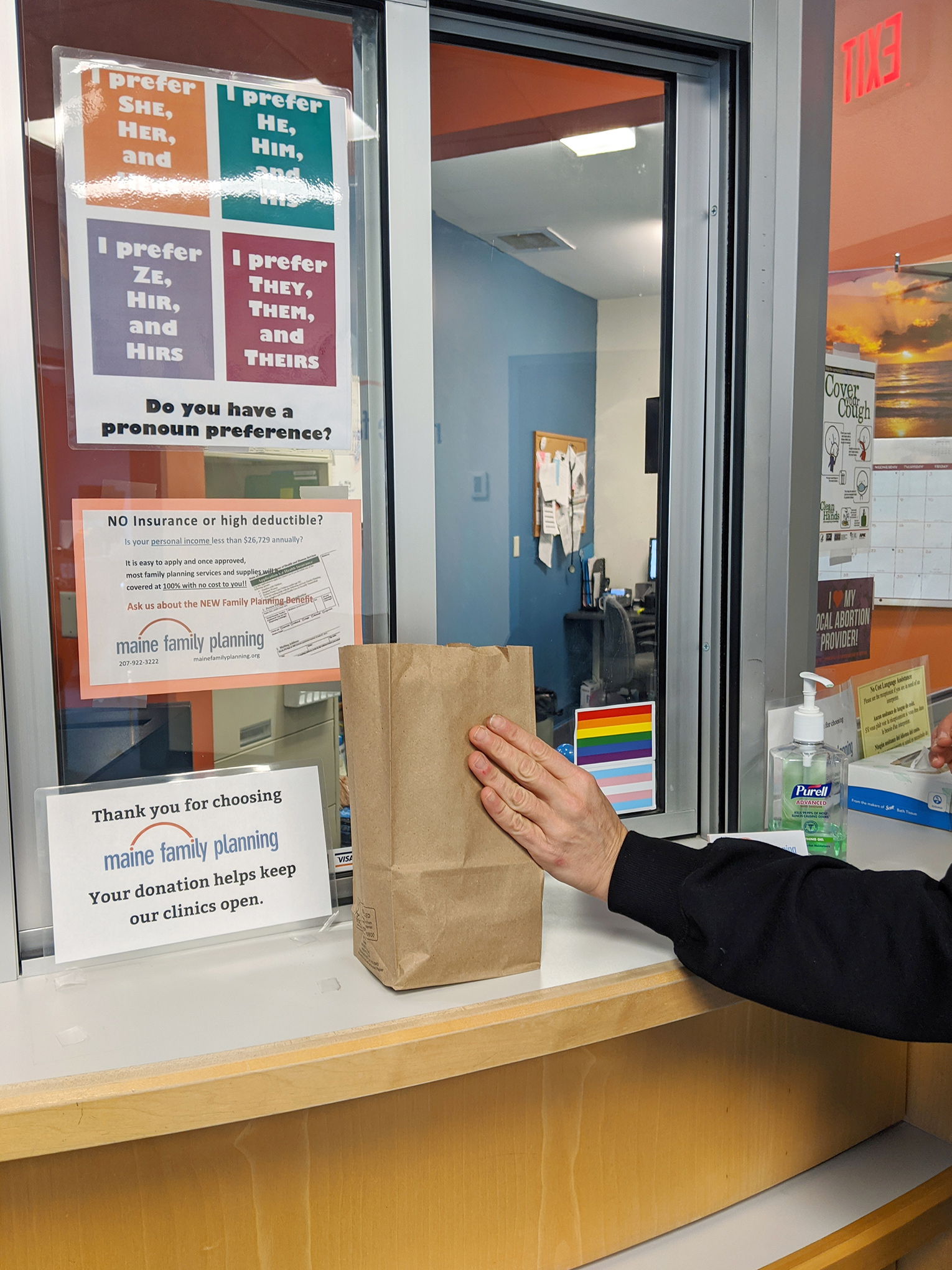
In late March, Leah Coplon, the program director at Maine Family Planning, watched as a young mother parked her car in front of the building. Carrying her baby, the mother was greeted by staff in the foyer and handed a brown paper bag that looked like a lunch sack. Then she loaded the bag and the baby into her car and drove away. Now she could end her pregnancy.
Less than two weeks earlier, on March 12, Maine had recorded its first case of COVID-19. Coplon knew this would make it harder for people to seek abortion services. Already elsewhere in the country, states were discussing shelter in place orders and medical supplies were in greater demand. She spent that weekend making plans for a program that would use the clinic’s existing telehealth setup to create a no-test, pick-up medication abortion service for patients with pregnancies of 10 weeks or less. This would limit human contact and the need for personal protective equipment in the clinic. On Monday, she smoothed out any wrinkles in the protocol with the National Abortion Federation. By Wednesday, March 18, Maine Family Planning launched its first contact-free, no-test abortion telehealth program, one of only a few in the country, at a time when abortion access is being threatened by conservative lawmakers as well as the increasing financial and social hardships caused by the pandemic.
Coplon’s urgency to jumpstart the program was not unfounded. In a matter of days, government officials in Texas, Ohio, Alabama, Oklahoma and Iowa would all identify abortion as a non-essential medical procedure that should be delayed or canceled amid the pandemic. Federal judges temporarily blocked some of these efforts, but the threat to abortion still looms. Leaders from 52 anti-abortion groups have signed a letter to the Secretary of Health and Human Services, urging public officials to restrict the operations of abortion providers to “free up much needed medical equipment” as well as “ensure that telemedicine abortion is not expanded during the crisis.”
Maine Family Planning’s program allows patients to receive the two medications necessary to complete an early abortion, without an in-person examination. For the young mother Coplon saw using the service in late March, the issue of finding someone to watch her baby, now that daycares and schools are closed due to the virus, was a huge barrier to getting the medical care she needed. Instead, she was able to go through an initial screening over the phone to determine if she was eligible for a medication abortion, followed by a telehealth visit with staff to review her available options, go through the informed consent process and receive instructions for care. After a telehealth visit with the clinician, she could simply pick up her pre-packaged medication, instructions and a home pregnancy test at one of 18 branches of the clinic around the state. One week later, she’d have a follow-up telehealth appointment to ensure everything went smoothly, and three weeks after that, she’d take the home pregnancy test to make sure the abortion was effective. The clinic has a 24/7 number where patients can reach out with any concerns.
“We feel that this both will reduce spread [of the virus] between patients and staff, allow us to have fewer people in the clinic so we are able to maintain social distancing as possible for patients, and to preserve our personal protective equipment which we need for aspiration abortions and which while right now is adequate, depending on how long this lasts, may become increasingly scarce,” says Coplon.
The spread of coronavirus has not only fueled the anti-abortion movement to limit clinic access, but it has also amplified existing issues that already made getting an abortion difficult. Poverty, which will likely skyrocket with the current unemployment numbers; access to transportation, much of which is shut down; and childcare difficulties, especially relevant considering about 60% of Americans receiving abortions are already mothers, are all exacerbated during the pandemic. “Maine struggles with some of the same issues that are national,” says Coplon. “A big issue now is that somebody being able to get an abortion while their kids were at school, now maybe have their kids at home.”
With even less consistent access to birth control now, some have predicted that the number of unplanned pregnancies might be on the rise, making access to abortion even more crucial. Since the program’s implementation, two-thirds of the center’s abortions have been no-test abortions, and the clinic has seen an increase in the total number of abortions requested compared to normal. Coplon believes that this small spike is due to patients trying to get abortions as soon as possible, stemming from rising concerns about clinics closing down.
The first telehealth medication abortion program in the U.S. began in 2008 in Iowa, but typically this type of program involved an initial in-person consultation and ultrasound to determine the gestational age of the embryo or fetus, along with any other necessary lab work. A physician would then review the results and medical history remotely and connect with the patient via telehealth. If eligible and the pregnancy was determined to be 10 weeks or less, the doctor would prescribe the abortion medication to the patient and watch them take the first of two pills over video conference. The second pill would be taken without supervision. Now, research has shown the safety and accuracy of using the date of a person’s last menstrual period to evaluate gestational age before taking medication abortion, eliminating the need for an ultrasound. One study published in Obstetrics & Gynecology found that the treatment is effective for up to 70 days of gestation, leaving some room for a margin of error. And in 2019, a bill was signed that allowed nurse practitioners, physician assistants and other qualified medical workers, not just doctors, in Maine to provide abortions independently.
After witnessing the success of the program, Coplon is hoping other clinics around the country will follow their lead, and participated in a webinar to discuss the program with other abortion providers. “There’s been a lot of interest in the protocol,” says Coplon. “There are folks from a lot of organizations that do research and practice in this area, who are working together to consolidate this protocol and get it out to as many folks as could use it. I do think that we’ll see a lot of clinics implementing this in the next few weeks.” But it will be impossible to expand the service nationwide. Currently, 18 states require the provider to be physically present during a medication abortion, effectively banning telemedicine abortions.
Further, by the end of June, some 58,000 family practice doctors are expected to cut back on services or shut down entirely, according to data from the American Academy of Family Physicians, and hospitals have already announced furloughs for more than 1,000 employees. In the wake of all this, patients in need of abortion services are living in anxiety.
“Oh good, you’re still open,” a patient calling to schedule an appointment said to Coplon when she answered the phone last week. “There is a relief I hear from patients when we answer the phone,” says Coplon. “Just letting folks know that we are here, that we have services and that we’re very committed to meeting their needs safely, and making sure that we can deliver that service with this minimal contact is necessary.” For the clinic’s patients, not having to chose between a virus and an unplanned pregnancy could be life-saving.
More Must-Reads from TIME
- Cybersecurity Experts Are Sounding the Alarm on DOGE
- Meet the 2025 Women of the Year
- The Harsh Truth About Disability Inclusion
- Why Do More Young Adults Have Cancer?
- Colman Domingo Leads With Radical Love
- How to Get Better at Doing Things Alone
- Michelle Zauner Stares Down the Darkness
Write to Anna Purna Kambhampaty at Anna.kambhampaty@time.com