
As we observe the 70th anniversary of the bombings of Hiroshima and Nagasaki, it may seem like the threat from nuclear weapons has receded. But it hasn’t; the threat is actually increasing steadily. This is difficult to face for many people, and this denial also means that we are not very well-prepared for nuclear and radiological events.
I’ve been studying the effects of nuclear events – from detonations to accidents – for over 30 years. I’ve been involved in research, teaching and humanitarian efforts in multiple expeditions to Chernobyl- and Fukushima-contaminated areas. Now I am involved in the proposal for the formation of the Nuclear Global Health Workforce.
Such a group could bring together nuclear and non-nuclear technical and health professionals for education and training, and help to meet the preparedness, coordination, collaboration and staffing requirements necessary to respond to a large-scale nuclear crisis.
Any nuclear weapon exchange or major nuclear plant meltdown will immediately lead to a global public health emergency. The Ebola outbreak taught the world that we should have resources in place to handle a major health emergency before it happens.
What would a Nuclear Global Health Workforce need to be prepared to manage? For that we can look back at the legacy of the atomic bombings of Hiroshima and Nagasaki, as well as the nuclear accidents like Chernobyl and Fukushima.
What happens when a nuclear device is detonated over a city?
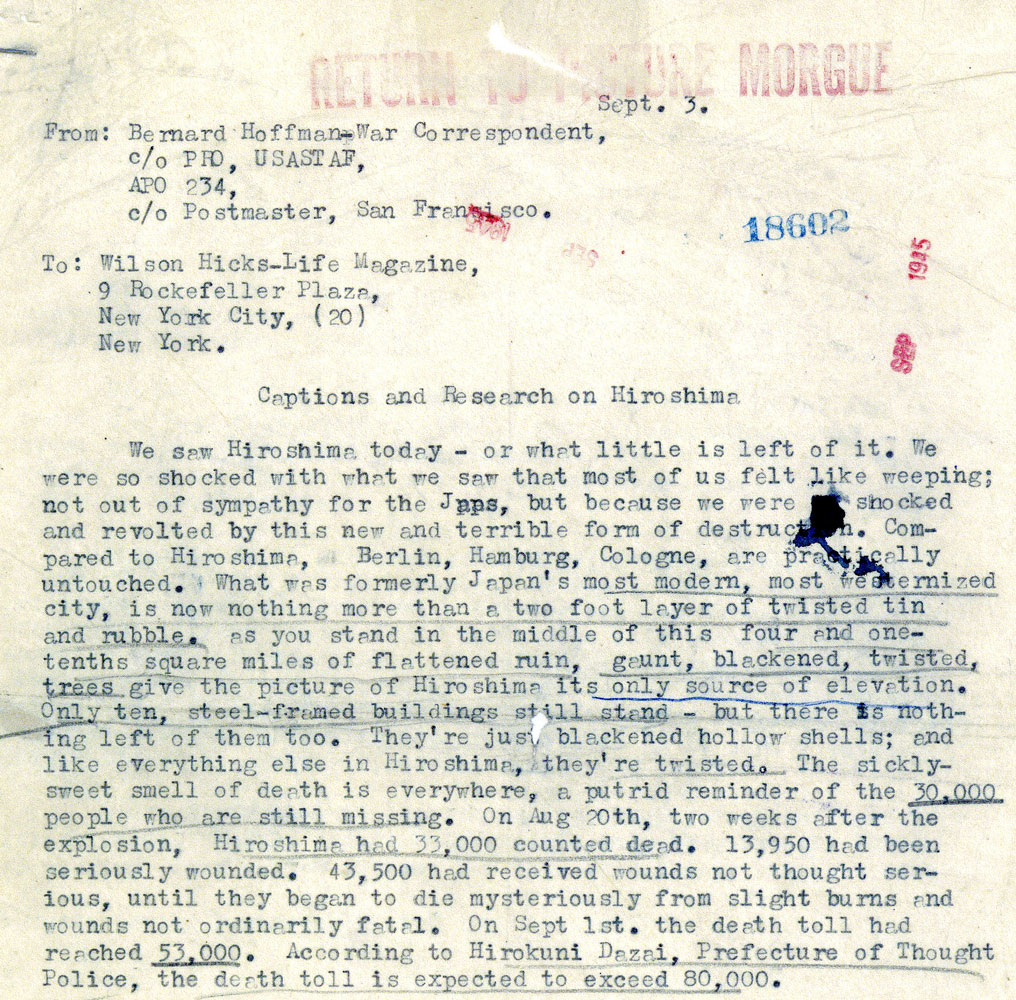
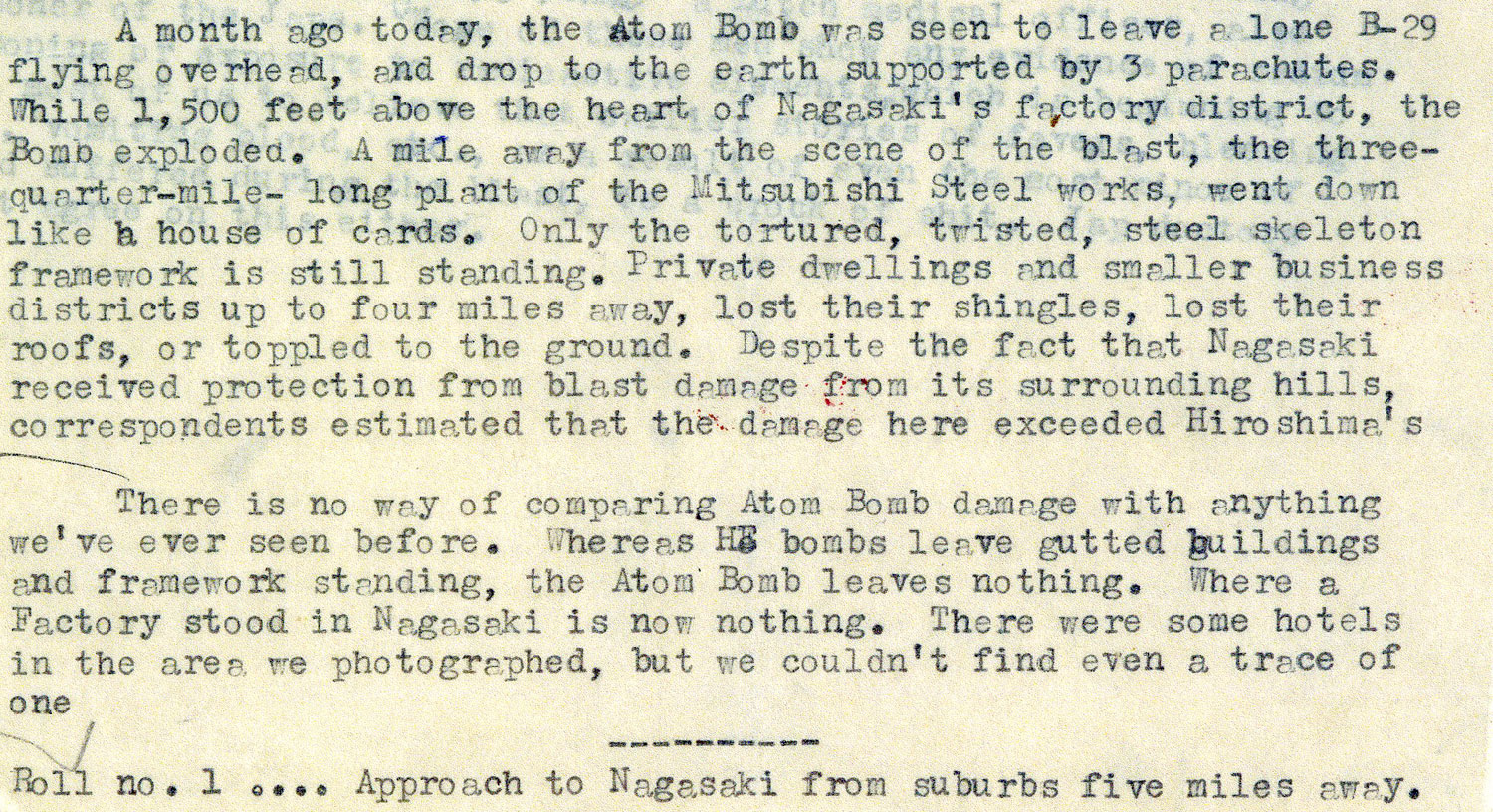
Approximately 135,000 and 64,000 people died, respectively, in Hiroshima and Nagasaki. The great majority of deaths happened in the first days after the bombings, mainly from thermal burns, severe physical injuries and radiation.
Over 90% of the doctors and nurses in Hiroshima were killed or injured, and therefore unable to assist in the response. This was largely due to the concentration of medical personnel and facilities in inner urban areas. This exact concentration exists today in the majority of American cities, and is a chilling reminder of the difficulty in medically responding to nuclear events.
What if a nuclear device were detonated in an urban area today? I explored this issue in a 2007 study modeling a nuclear weapon attack on four American cities. As in Hiroshima and Nagasaki, the majority of deaths would happen soon after the detonation, and the local health care response capability would be largely eradicated.
Models show that such an event in an urban area in particular will not only destroy the existing public health protections but will, most likely, make it extremely difficult to respond, recover and rehabilitate them.
With medical facilities decimated after a detonation, treating the injured will be a tremendous challenge. We would need predicted casualty distributions and locations to figure out how to best allocate what resources and personnel remain.
Very few medical personnel today have the skills or knowledge to treat the kind and the quantity of injuries a nuclear blast can cause. Health care workers would have little to no familiarity with the treatment of radiation victims. Thermal burns would require enormous resources to treat even a single patient, and a large number of patients with these injuries will overwhelm any existing medical system. There would also be a massive number of laceration injuries from the breakage of virtually all glass in a wide area.
Currently, it has not been worked out how medical systems in affected areas are supposed to cope with the overwhelming numbers of patients from an urban nuclear detonation. This makes it that much more important to have an effort like the Nuclear Global Health Workforce to work to address and help nations prepare for these overwhelming events.
Getting people out of the blast and radiation contamination zones
A major nuclear event would leave large swaths of territory uninhabitable for decades, with catastrophic impacts on humans, the economy and the environment.
Decisions to evacuate at-risk populations must be made within hours, but plans for and criteria to evacuate are lacking. And the scale of these evacuations and potential resettlement is tremendous.
For instance, within a few weeks after the Chernobyl accident, more than 116,000 people were evacuated from the most contaminated areas of Ukraine and Belarus. Another 220,000 people were relocated in subsequent years. But thousands continue to live in areas classified by Ukrainian and Belarussian authorities as strictly controlled zones, where chronic radioactive cesium contamination remains a problem.
The day after the Fukushima earthquake and tsunami, over 200,000 people were evacuated from areas within 20 kilometers (12 miles) the nuclear plant because of the fear of the potential for radiation exposure.
On Day 3, people living in the 20-30 kilometer (12-18 mile) zone around the plant were asked to remain indoors, and eventually advised to self-evacuate.
The evacuation process was plagued by misinformation, inadequate and confusing orders and delays in releasing information. There was also trouble evacuating everyone from the affected areas. Elderly and infirm residents were left in areas near the plant, and hospitalized patients were not always taken where they needed to go. All of these troubles lead to a loss of public trust in the government.
Chernobyl and Fukushima were both reactor meltdowns. A high-yield nuclear weapon – that is, a large device with a very large blast and radiation capability – would bring patient and evacuation numbers to incomprehensible levels.
However, the current Department of Homeland Security most-anticipated scenario for a nuclear attack in the US is for smaller nuclear weapons – 10 kilotons – about the size of the weapons used to attack Hiroshima and Nagasaki.
And new evidence has altered previous dire predictions in relatively low-yield nuclear blasts such as Hiroshima and Nagasaki. Current US nuclear war response protocols do not rely as much on large-scale evacuations from nearby areas.
For instance, in a hypothetical low-yield (10 kiloton) nuclear bomb over Washington DC, only limited evacuations are planned. Despite projections of 100,000 fatalities and about 150,000 casualties, the casualty-producing radiation plume would actually be expected to be confined to a relatively small area. People upwind would not need to take any action, and most of those downwind, in areas receiving relatively small radiation levels (from the point of view of being sufficient to cause radiation-related health issues), would need to seek only “moderate shelter.”
A Nuclear Global Health Workforce could start to lay out plans for how to rapidly respond to such an attack and project whether and what sort of evacuation plans would be needed.
The long-term effects of radiation exposure
The Radiation Effects Research Foundation (RERF), which was established to study the effects of radiation on survivors of the Hiroshima and Nagasaki, has been tracking the health effects of radiation for decades.
According to RERF, about 1,900 excess cancer deaths can be attributed to the atomic bombs, with about 200 cases of leukemia and 1,700 solid cancers. Japan has constructed very detailed cancer screenings after Hiroshima, Nagasaki and Fukushima; Chernobyl research has also been extensive, but not to the extent as in ongoing in Japan.
But the data on many potential health effects from radiation exposure, such as birth defects, arere less conclusive.
While it has been shown that intense medical X-ray exposure has accidentally produced birth defects in humans, there is considerable debate about whether there were birth defects in the descendants of Hiroshima and Nagasaki atomic bomb survivors.
For example, one study found more than a doubling of brain malformations in some children from Hiroshima and Nagasaki, while other respected long-term investigations have concluded there are no statistically significant increases in birth defects resulting in atomic bomb survivors.
Looking at data from Chernobyl, where the release of airborne radiation was 100 times as much as Hiroshima and Nagasaki combined, there is a similar lack of definitive data for radiation-induced birth defects.
A wide-ranging WHO study concluded that there were no differences in rates of mental retardation and emotional problems in Chernobyl radiation-exposed children compared to children in control groups.
A Harvard review on Chernobyl concluded that there was no substantive proof regarding radiation-induced effects on embryos or fetuses from the accident. Another study looked at the congenital abnormality registers for 16 European regions that received fallout from Chernobyl, and concluded that the widespread fear in the population about the possible effects of radiation exposure on the unborn fetus was not justified.
Indeed, the most definitive Chernobyl health impact in terms of numbers was the dramatic increase of elective abortions near and at significant distances from the accident site. This was due to “nuclear phobia,”, lack of information and inadequate official guidance. Not having been informed about the actual lack of risk, there was understandable anxiety regarding the possible effects of radiation on the fetus, and a panic among expectant mothers about giving birth to a child with a birth defect.
A Nuclear Global Health Workforce could help health care practitioners, policymakers, administrators and others understand myths and realities of radiation. In the critical time just after a nuclear crisis, this would help officials make evidence-based policy decisions and help people understand the actual risks they face.
What’s the risk of another Hiroshima or Nagasaki?
Today, the risk for a nuclear exchange – and its devastating impact on medicine and public health worldwide – has only escalated. Nuclear weapons are spreading to more nations, and international relations are increasingly volatile. The developing technological sophistication among terrorist groups and the growing global availability and distribution of radioactive materials are also especially worrying.
Despite the gloomy prospects of health outcomes of any large scale nuclear event common in the minds of many, it is our mutually shared moral and ethical obligation to respond.
Cham Dallas is Professor and Director, Institute for Disaster Management at University of Georgia.
This article was originally published on The Conversation. Read the original article.
Hiroshima and Nagasaki: Photos From the Ruins














More Must-Reads from TIME
- Donald Trump Is TIME's 2024 Person of the Year
- Why We Chose Trump as Person of the Year
- Is Intermittent Fasting Good or Bad for You?
- The 100 Must-Read Books of 2024
- The 20 Best Christmas TV Episodes
- Column: If Optimism Feels Ridiculous Now, Try Hope
- The Future of Climate Action Is Trade Policy
- Merle Bombardieri Is Helping People Make the Baby Decision
Contact us at letters@time.com